
Opinion|Videos|November 3, 2023
Cross Q&A: Retrospective Study of Patients With MM
Experts in the field of multiple myeloma discuss data from a retrospective study on patients with multiple myeloma.
Advertisement
Episodes in this series



Transcript:
Judy Schreiber, PhD, RN: Over to you, Cleveland Clinic, for comments and questions.
Faiz Anwer, MD, FACP: This was a great presentation, and you are right about showing the comparison with the study. We did an analysis in our practice here with 500 patients, and we saw very similar patterns of outcome with patients who progressed with either biochemical relapse or clinical relapse. So thank you.
Jack Khouri, MD: Yes, I agree. So, Jeff, how is this going to change your practice? Are you going to do anything differently based on this?
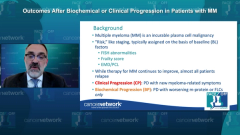
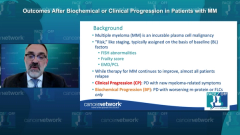
Jeffrey Zonder, MD: I mean, that’s the thing. This kind of confirms, I think, what many of us already know, right? It’s really the patient’s baseline characteristics.
You know, whether it’s high-risk FISH [fluorescence in situ hybridization], extramedullary disease, or circulating plasma cells, at diagnosis, we already know those patients clinically do worse to the point that we often [treat them] differently along the way in terms of their maintenance therapy. And the therapies we’re currently using aren’t the therapies that were used in this retrospective data set. These are patients who were treated and diagnosed prior to 2018. So these aren’t Dara [daratumumab]-treated patients, by and large. Most of them aren’t getting doublet maintenance therapy for high-risk disease.
So I’m not sure that it changes anything. I think our [treatment of] high-risk patients has already moved past what was being done in this particular study. It does also, however, remind us that [for] biochemical progressors, you can afford to watch them sometimes as long as you pay attention to biochemical progression always. Biochemical progression should trigger reimaging. This study showed us that bone lesions are the way that it sneaks up on us clinically. So as long as you’ve reassured yourself that it’s really just biochemical, you can sometimes let an indolent biochemical progression go for a little while in a patient who’s tolerating therapy before moving on to the next line of treatment.
Moaath Mustafa Ali, MD, MPH: Dr Zonder, thank you for this nice presentation. I have a question about the study design. Now, patients who had clinical progression vs biochemical progression in the biochemical progression, did that group of patients only include patients who have never had a clinical progression vs only having a biochemical progression at their first progression?
Because there’s a difference, if it was only biochemical vs only at the first progression.
Jeffrey Zonder, MD: These were all patients being analyzed for first progression.
Moaath Mustafa Ali, MD, MPH: For the first progression?
Jeffrey Zonder, MD: This is just the first progression. So the progression was categorized as either biochemical or clinical, based on whether or not they developed new CRAB [carbapenem-resistant Acinetobacter baumannii].
They defined it in the paper, but basically [it meant] new or growing plasmacytomas or bone lesions, worsening anemia by 2 gm, a drop below 10 [gm], or a change in renal function. This was spelled out in the paper, but they defined what clinical progression entailed.
Moaath Mustafa Ali, MD, MPH: I have another question for you, or another observation. When I was looking at the table, you showed the odds ratio for
presentation compared with the relapse. It was interesting that patients who had renal disease at the time of presentation only relapsed with, or they only progressed with, renal disease. There was no association with other diseases. I don’t know if you have any thoughts about that, but do these [patients have disease that behaves] differently, biologically, compared with other subtypes of multiple myeloma?
Jeffrey Zonder, MD: I’m not 100% sure, you know, that was hard to tease apart.… I’d have to go back to the demographics table, but I don’t believe, for instance, that we know, what percentage of these patients were light chain only; I don’t know that.
It wouldn’t be surprising if the light chain levels were different for those patients who presented originally with renal insufficiency. If they had a disproportionate number of patients who were light chain only or had extremely high light chains at presentation, it wouldn’t be that surprising when they progressed. That’s how they know that was the manifestation of their progression.
Transcript is AI-generated and edited for clarity and readability.
Newsletter
Stay up to date on recent advances in the multidisciplinary approach to cancer.
Advertisement
Related Content





Latest CME














































Advertisement
Advertisement
Trending on CancerNetwork
1
FDA Approves Vepdegestrant in ER+, HER2–, ESR1-Mutated Breast Cancer
2
FDA Permits Expanded Daraxonrasib Access in Previously Treated Metastatic PDAC
3
FDA ODAC Votes Yes to Capivasertib for PTEN-Deficient Metastatic HSPC
4
FDA ODAC Votes No to Camizestrant for HR+/HER2– ESR1 Advanced Breast Cancer
5