Articles by Shandra S. Wilson, MD
A 70-year-old man presented at our institution for a second opinion regarding diagnosis of a urinary bladder mass. He had a 3-year history of worsening urinary incontinence and urgency, for which he had undergone colonoscopy, as well as testing for prostate issues; all test results were negative.
Lymphoepithelioma-Like Carcinoma of the Urinary Bladder
ByElizabeth R. Kessler, MD,Arya Amini, MD,Shandra S. Wilson, MD,Kathryn Breaker, RN-MS, ANP-C,David Raben, MD,Francisco G. La Rosa, MD,E. David Crawford, MD A 65-year-old woman presented to a local emergency department complaining of right flank pain that had worsened over the past 10 days. A CT scan of the abdomen and pelvis showed intravesical tumors of the urinary bladder.

A Rare Case of Metastatic Renal Epithelioid Angiomyolipoma
ByElaine T. Lam, MD,Francisco G. La Rosa, MD,Thomas D. Suby-long, MD,Kimi L. Kondo, DO,Shandra S. Wilson, MD,L. Michael Glodé, MD, FACP,Thomas W. Flaig, MD The patient is a 43-year-old man who was initially evaluated at an outside institution for unexplained anemia and who was found to have a large right kidney mass. He underwent a radical nephrectomy for a 19-cm large-cell, poorly differentiated neoplasm, consistent with pleomorphic, epithelioid angiomyolipoma (EAML) with extensive necrosis and cytologic atypia.
The authors on “Solitary Extramedullary Plasmacytoma of the Bladder” have provided a quick and accurate diagnosis, work-up, and treatment of this solitary extramedullary plasmacytoma. Solitary extramedullary plamacytomas are rare, and account for only 3% of all plasma cell malignancies. Of the 3% of plasma cell malignancies that are diagnosed, the bladder is one of the least common locations. The rarity of the tumor frequently makes the process of making a correct diagnosis difficult.[1] After making the diagnosis with immunohistochemistry, a bone marrow biopsy must be performed to rule out multiple myeloma. Additionally, a body and skeletal survey must show no evidence of additional disease or lytic lesions in order to confirm localized disease. In this case, these procedures were performed accurately and in a timely fashion.
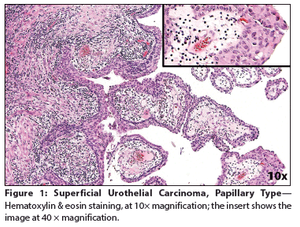
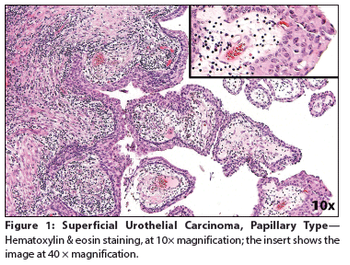
Recurrent Urothelial Carcinoma With Pulmonary Metastasis
ByVassilis J. Siomos, MD,Francisco G. La Rosa, MD,Thomas W. Flaig, MD,Kimi L. Kondo, DO,John D. Mitchell, MD,Shandra S. Wilson, MD A 56-year-old woman was referred to our institution for a left nephroureterectomy after the diagnoses of a nonfunctioning left kidney and noninvasive papillary urothelial carcinoma of the distal left ureter (Ta grade 1). Following the procedure, surveillance cystoscopy and computed tomography (CT) scan of the abdomen and pelvis demonstrated a large bladder tumor with pan-urothelial extension.

The patient is a 39-year-old man who presents with pelvic lymphadenopathy. He has a history of ureteral reflux disease, recurrent nephrolithiasis, right nephrectomy, ileal loop diversion of the left ureter, and radical cystectomy for “bladder cancer,” which he underwent 3 years ago. The lymphadenopathy was discovered incidentally during recent imaging.
The patient is a 39-year-old Caucasian male who presented with a right renal mass and painless gross hematuria. He underwent a right laparoscopic radical nephrectomy and the final pathology revealed a carcinoid tumor.