

































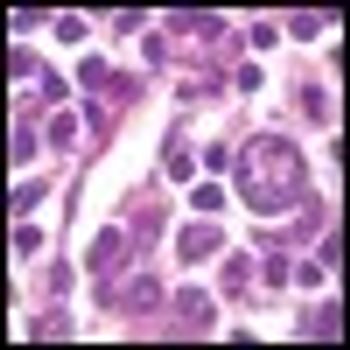
In their article in this issue of ONCOLOGY, Nastoupil, Rose, and Flowers give a very careful assessment of the options for treating diffuse large B-cell lymphoma (DLBCL), with a focus on the importance of dose density in improving outcomes in this disease.
Lymphoma
Latest News
Advertisement
CME Content
Advertisement
This article examines clinical and biological features of DLBCL patients with poor outcomes, and reviews recent studies addressing alternatives to standard front-line management strategies together with unresolved questions.

This review addresses the rationale and evidence for-and the challenges, cost implications, and future development of-proton therapy as an important part of the treatment strategy in Hodgkin lymphoma.
Leukemias and lymphomas are estimated to contribute up to 7% of all new malignant cases in the United States.[1]
The leukemias and lymphomas represent a group of heterogeneous myeloid or lymphoid clonal stem cell disorders with variable clinical presentation, pathological characteristics, prognosis and recommendations for treatment.[1]
The management of leukemias and lymphomas now includes the use of many targeted therapies. Nurses need to have an understanding of the targeted therapies and their side effects so they can appropriately manage the side effects that their patients with leukemias and lymphomas may experience.
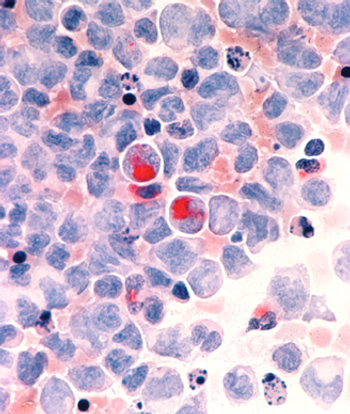
Two researchers from the Mayo Clinic have published an editorial calling for new approaches in the treatment of AML, arguing that "using the same old drugs in different doses or different schedules is not going to cut it."
Cancer treatment is undergoing significant developments and entering the new golden era of genomics which has true potentials for the promise of personalized medicine. Large-scale sequencing is changing our understanding of malignant disorders particularly acute myeloid leukemia.
Inotuzumab ozogamicin has achieved a markedly long antitumor response in patients with refractory or relapsed indolent B-cell non-Hodgkin lymphoma (NHL) in an ongoing phase II study. Interim findings were reported by lead investigator Kenneth Luu, PhD, associate director of Pfizer global R&D.
A combination of TL32711, an investigational second mitochondrial-derived activator of caspases (Smac), and tumor necrosis factor-related apoptosis inducing ligand at low concentrations produced marked apoptosis in germinal center lines, with minimal to no effect for each agent alone.
Preliminary findings of a phase I/II randomized clinical trial indicate that SGI-110, a novel DNA methylation inhibitor, is safe, well tolerated and efficacious in patients with acute myelogenous leukemia.
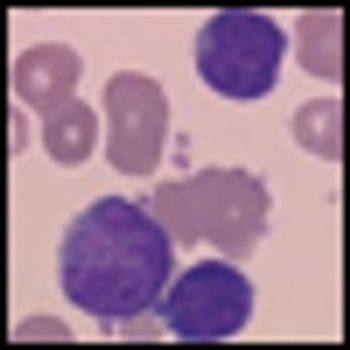
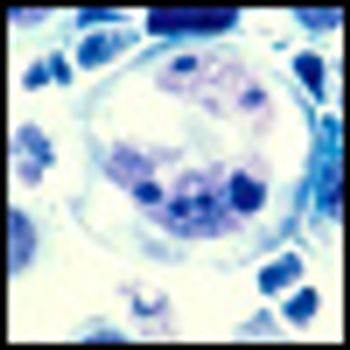
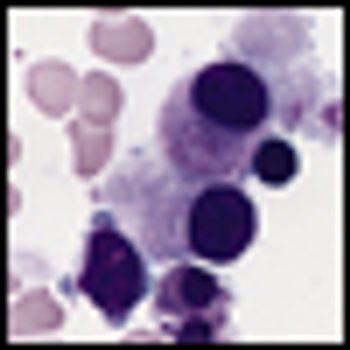
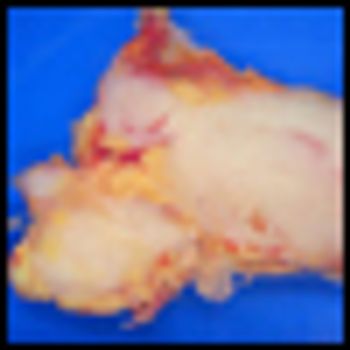
In this article, we review the current knowledge on the biological findings, clinical features, and therapeutic approaches for splenic marginal zone lymphoma.

Four publications on cancer treatment during pregnancy were published last week in the journal Lancet, serving as new treatment guidelines for chemotherapy and surgery in pregnant patients with solid tumors and hematologic malignancies.
Splenic lymphomas are a diverse group of lymphoid malignancies that have clinical behavior ranging from indolent to aggressive and that have both B-cell and T-cell histologies.
The article by Thieblemont and colleagues very nicely summarizes the key pathogenetic and diagnostic features and present treatment of splenic marginal zone lymphoma (SMZL).
Until we fully engage in understanding the biologic mechanisms that separate NMZL from other indolent NHLs, however, we will continue to deliver “impersonalized medicine” that does not exploit the unique properties of the former.
Typically, when one authors a commentary piece, a good template to follow is to start with some background material, review the major findings of the paper in question, and then focus on areas of controversy and unanswered questions.
The aim of this review is twofold: to summarize descriptions of the clinical presentation provided in published series in order to help clinicians recognize and treat patients, and to discuss diagnostic difficulties faced by hematopathologists when dealing with these lesions and others in the differential diagnosis that must be distinguished from one another.

The results of the 2-year follow-up of the dasatinib DASISION phase III trial show the continued superiority of the drug compared to imatinib. The results provide further support for treatment of first-line chronic phase chronic myeloid leukemia patients that harbor the Philadelphia chromosome.
Results of the phase III SWOG S0016 trial comparing 2 chemotherapy regimens for follicular lymphoma (FL), presented this week at ASH, show no statistically significant differences in either progression-free survival (PFS) or overall survival. Both regimens produced “excellent” results, according to the presenter.

The phase III randomized RESORT (ECOG Protocol E4402) trial asked whether a maintenance schedule of rituximab every 3 months would lead to a superior disease control outcome compared to retreatment upon progression. The answer, presented this week at ASH, is no.

The phase III trial comparing the use of gemtuzumab ozogamicin combined with chemotherapy to chemotherapy alone in newly diagnosed acute myeloid leukemia (AML) patients provides evidence that the combination treatment may be promising in this patient population.

Obinutuzumab (GA101) achieved higher response rates than rituximab in the first head-to-head trial of the two biologic agents in patients with relapsed non-Hodgkin lymphoma.
Encouraging findings were reported from multiple studies of ibritumomab tiuxetan (Zevalin), a CD20-directed radiotherapeutic antibody, in diverse patient groups with follicular lymphoma.

Andrew Evens, DO, MSc, deputy director for clinical and translational research and medical director of the Clinical Research Office at the UMass Memorial Health Care Cancer Center of Excellence, talks about his research on lymphoma during pregnancy.
Advertisement
Advertisement
Trending on CancerNetwork
1
Modifiable Risk Factors Suggest Potential for Improving Cancer Prevention
2
2026 Tandem Meetings: What’s the Latest Research in Multiple Myeloma?
3
Dato-DXd Receives Priority Review in Unresectable/Metastatic TNBC
4
Barriers to CAR T-Cell Referral and Center Access in Multiple Myeloma
5