
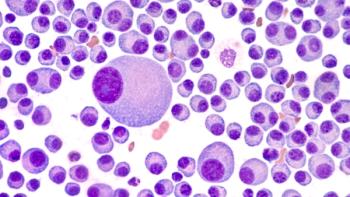
Short discussed currently available assays for MRD detection, blinatumomab treatment, and other implications from an ALL study presented at the 2020 ASH Annual Meeting.

Your AI-Trained Oncology Knowledge Connection!
Short discussed currently available assays for MRD detection, blinatumomab treatment, and other implications from an ALL study presented at the 2020 ASH Annual Meeting.

The results of one study suggested that older adults with advanced cancer may be at a higher risk for financial toxicity compared with those undergoing treatments for other chronic conditions.

Ghobadi detailed the next steps needed to build on the results of a study presented at the 2020 American Society of Hematology Annual Meeting & Exposition.

“These findings suggest that similar to its benefits in ovarian cancer, NACT could potentially lower perioperative morbidity and may serve as an important treatment option among women with metastatic endometrial cancer,” the study authors wrote.
Wolf touched on the implications of results from a study investigating outcomes when making clinical decisions based on the MRD status of patients with multiple myeloma.

This study indicated that appendiceal cancer diagnosed among younger individuals harbors a distinct genomic landscape, as compared with appendiceal cancer diagnosed among older individuals.

A study of the effect of intravenous immunoglobulin (IVIG) on infections in patients with multiple myeloma receiving daratumumab indicated that hypogammaglobulinemia was nearly universal during treatment, suggesting a role for IVIG.

Vikram Narayan, MD, expanded on his data regarding nadofaragene and NMIBC published at this year’s SUO Meeting.
The leukemia expert offered an overview of agents approved by the FDA this year.

Extended follow up and preliminary findings from an extension cohort of the GO29365 study of polatuzumab vedotin (Polivy) for patients with diffuse large B-cell lymphoma confirmed earlier reports of efficacy and safety, and demonstrated continued deepening responses.
The phase 2 HORIZON study indicated that melflufen plus dexamethasone (Ozurdex) demonstrated clinically meaningful efficacy as well as a manageable safety profile in patients with heavily pretreated relapsed/refractory multiple myeloma.
Dan Pollyea, MD discusses the response rate and overall survival of venetoclax for patients with acute myeloid leukemia with IDH mutations.

Declan Murphy discusses the accuracy findings from the proPSMA study presented at the 2020 SUO Meeting.
Study results indicated that MK-6482 demonstrated durable efficacy in patients with Von Hippel-Lindau disease-associated clear cell renal cell carcinoma, pancreatic lesions, and hemangioblastomas by targeting the underlying pathophysiology of the disease.

The director of clinical research in the Center for Cancer Care at White Plains Hospital explained the design of the study which evaluated diabetic versus nondiabetic patients enrolled in the CONNECT Multiple Myeloma Registry.

Given the limited success and potential harms associated with pharmacological interventions, the researchers suggested that nonpharmacological interventions such as those identified in the study should be considered as first-line treatment options for managing breathlessness.
The expert from the Levine Cancer Institute discussed the findings from an updated analysis of the phase 2 GRIFFIN Trial for patients with newly diagnosed multiple myeloma.

The Emory University Winship Cancer Institute expert discussed FDA approvals and other treatment advances that occurred this year.

This study found that among patients with lung cancer from Latin America, Native American ancestry was associated with increased mutations in the EGFR gene, independent of smoking status.

“In the long-term, active surveillance is a safe and viable option for men with low-risk and carefully selected intermediate-risk prostate cancer,” the study authors wrote.
The latest episode of the “Oncology Peer Review On-The-Go” podcast discusses a review article on patient-reported outcomes of cancer-related pain.

The study was designed to determine the impact of a rurally focused telemedicine program on patient outcomes.

Short summarized the NGS-based MRD findings from his ALL study presented at the 2020 ASH Annual Meeting.

This new risk estimation model could help physicians determine whether an average risk patient’s specific risk indicates an at-home stool test would be a good screening option or suggests a colonoscopy may be the most appropriate option.

Narayan expanded on the other studies he contributed to from SUO investigating nadofaragene for patients with NMIBC.
Based on the recommendation of an independent data monitoring committee, Astellas has halted enrollment in the trial and is reviewing the results for further actions needed.

Though these collective findings demonstrate that genetic predisposition to increased weight is protective against breast and prostate cancer, further research is still necessary to work out exactly how this protection is provided, especially in breast cancer.
Ghobadi explained an interesting correlation found in the results of his study presented at the 2020 ASH Annual Meeting & Exposition.
Digital breast tomosynthesis plus synthetic mammography depicted more cancers and found a lower number of stage II cancers at repeat screening compared with FFDM.
Wolf discussed the decisions to change therapy based on the MRD status of patients with multiple myeloma.